Minimally Invasive Resin Build-up Is the Answer for Pediatric Cavities — Treating Extensive Secondary Caries in a 9-Year-Old
A 9-year-old patient's lower first molar (#46) had a failed previous resin restoration with extensive secondary and subgingival caries. Treated with gum recontouring, rubber dam isolation, AquaCare, and fiber-reinforced resin build-up using a minimally invasive approach.
Patient Information
9 years old
#46 Failed resin restoration, secondary & subgingival caries
Hello. I'm Dr. Kang Seokhoon, Director of Shin Youngtong TTE Dental Clinic — a practice that never gives up on saving natural teeth.
Today's case is about treating a cavity in the lower first molar (#46) of a 9-year-old child. The patient came in for a routine checkup, and we discovered extensive secondary caries hidden beneath a previous resin restoration done at another clinic.
"My child needs a crown on a baby — I mean, permanent tooth?"
"Wouldn't an inlay be better?"
These are the most common questions parents ask. The bottom line: for children and adolescents, we recommend minimally invasive resin build-up over more aggressive treatments like crowns or inlays. Here's why, illustrated with the actual treatment process.
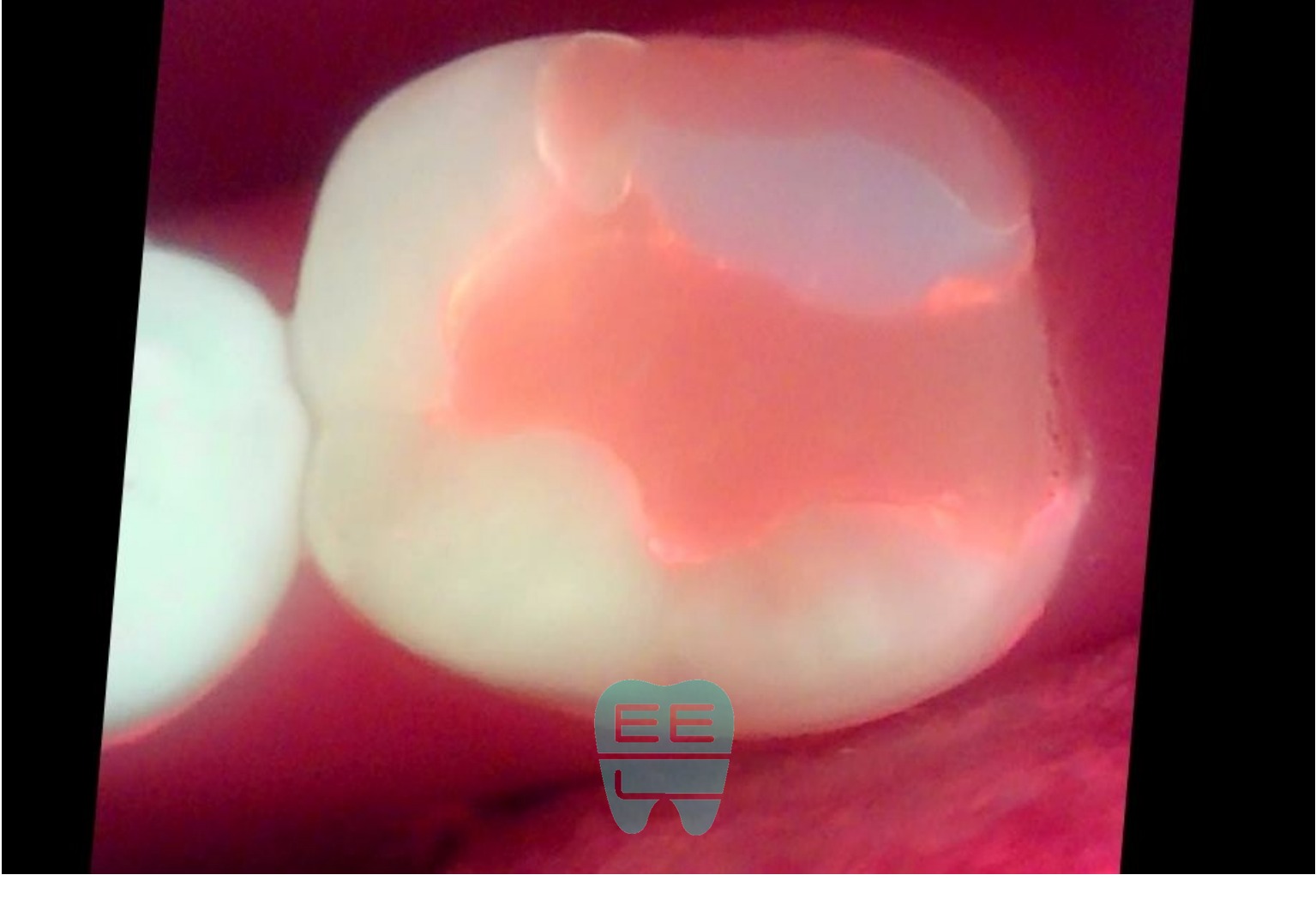
1. Initial Examination: Looks Fine on the Surface, But...

This is what the tooth looked like at the first visit. At first glance, the existing resin restoration seems fine. But on closer inspection, the resin was debonding and lifting away from the tooth.
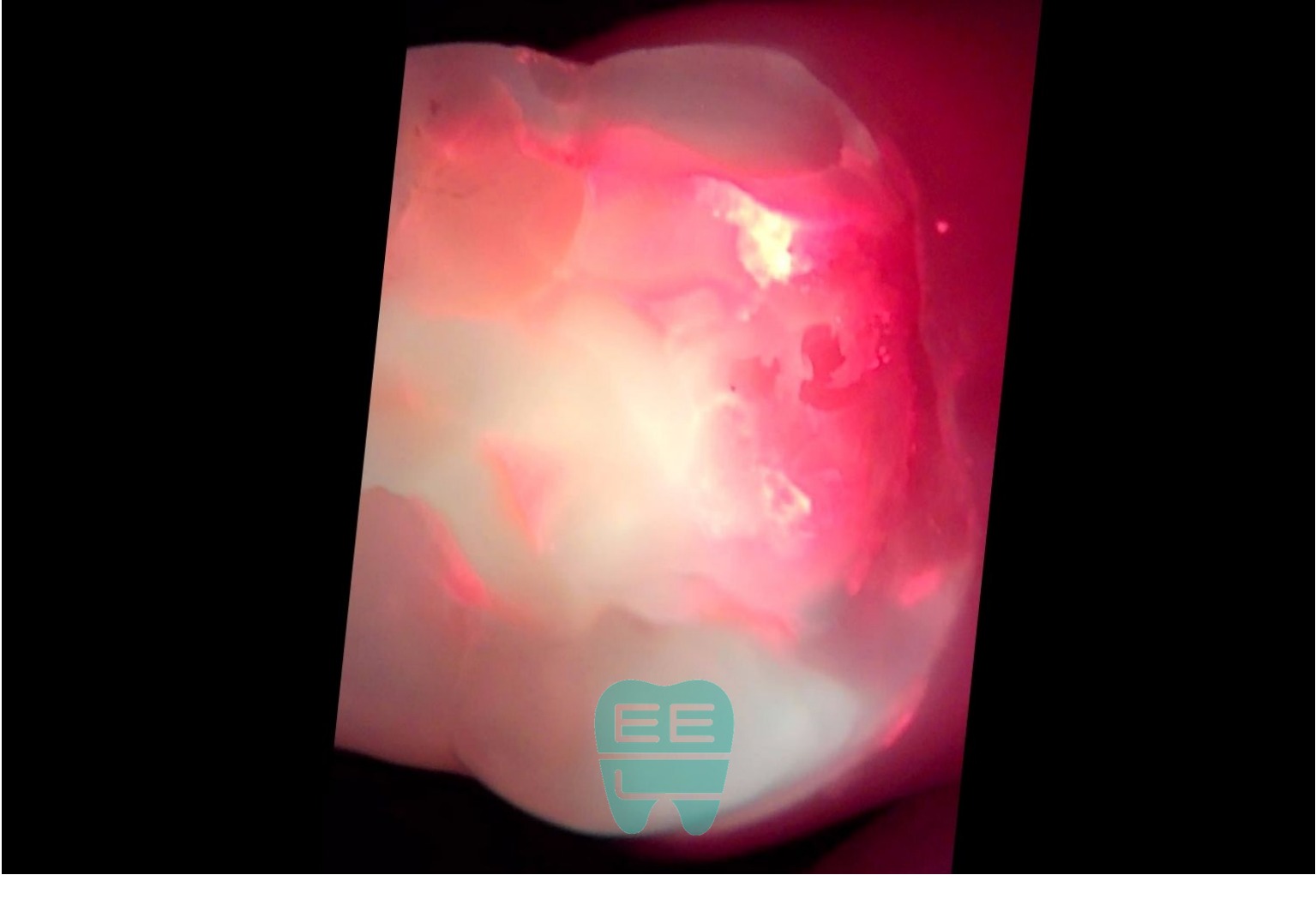
2. Q-ray (QLF) Examination: Revealing Hidden Decay
Q-ray (QLF — Quantitative Light-induced Fluorescence) uses special fluorescence to visualize invisible cavities and bacterial contamination. The red-colored areas indicate bacterial contamination and decay — extensive contamination is visible beneath the existing resin.
The surface looked fine, but inside, things were already serious.
3. Removing the Old Resin: Worse Than Expected

When removing the old resin, the bonding had completely failed — it just popped right off. Underneath was extensive secondary caries and decay that had progressed below the gum line (subgingival caries).
Proper rubber dam placement required gum recontouring (gingivectomy) first, as the decay extended beneath the gum tissue.
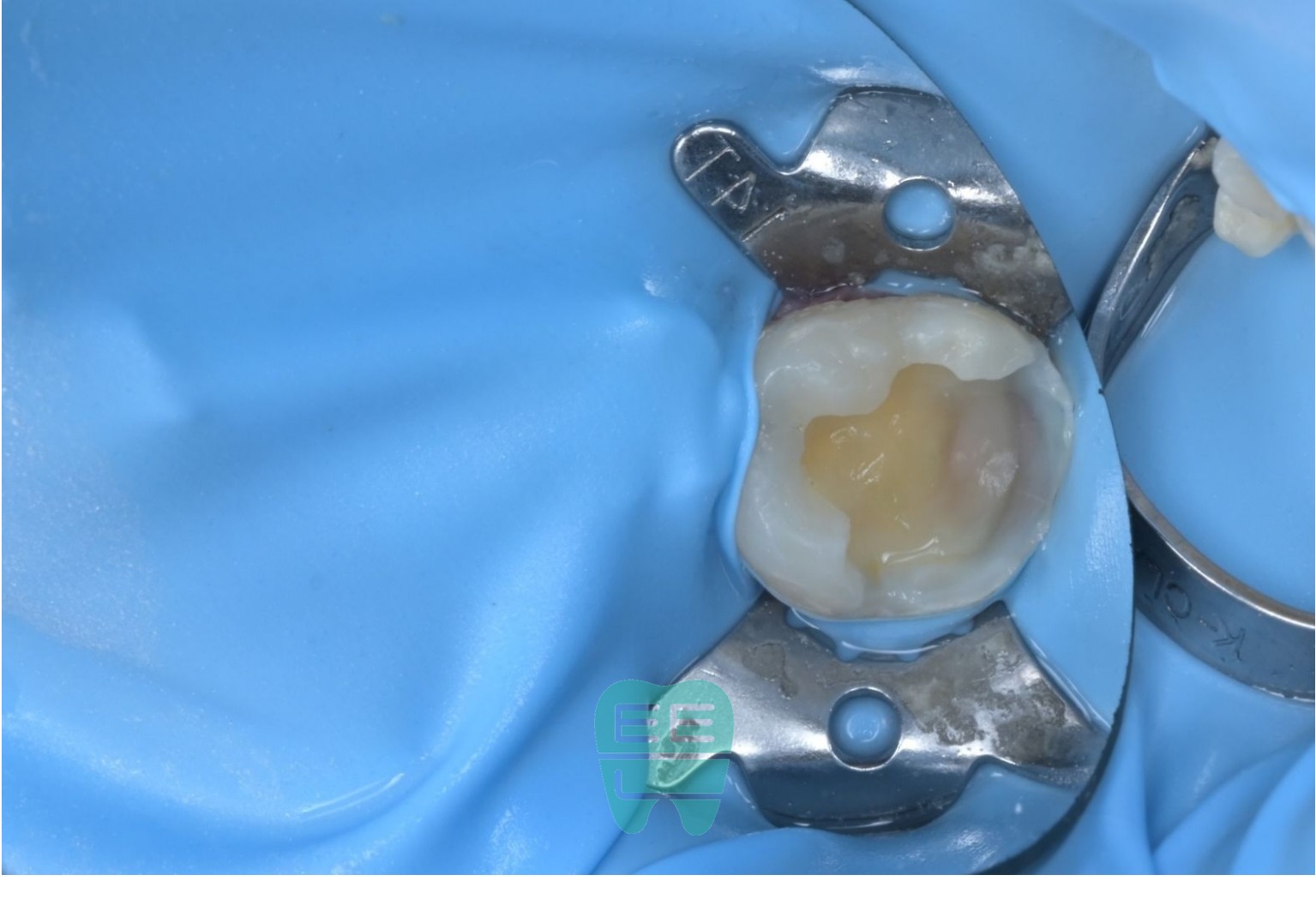
4. Rubber Dam Placement: The Key to Successful Treatment

The success of cavity treatment ultimately depends on how well you can maintain a dry field. After recontouring the gums with a laser to expose the tooth margins, we placed the rubber dam.
The rubber dam prevents saliva and blood from contaminating the treatment area, allowing the adhesive to perform at its maximum potential. For pediatric patients, rubber dam isolation is even more critical since saliva control is more difficult.
5. Tracking Decay Removal with Q-ray
After completely removing the old restoration, Q-ray imaging shows severe contamination (red fluorescence) throughout the area.
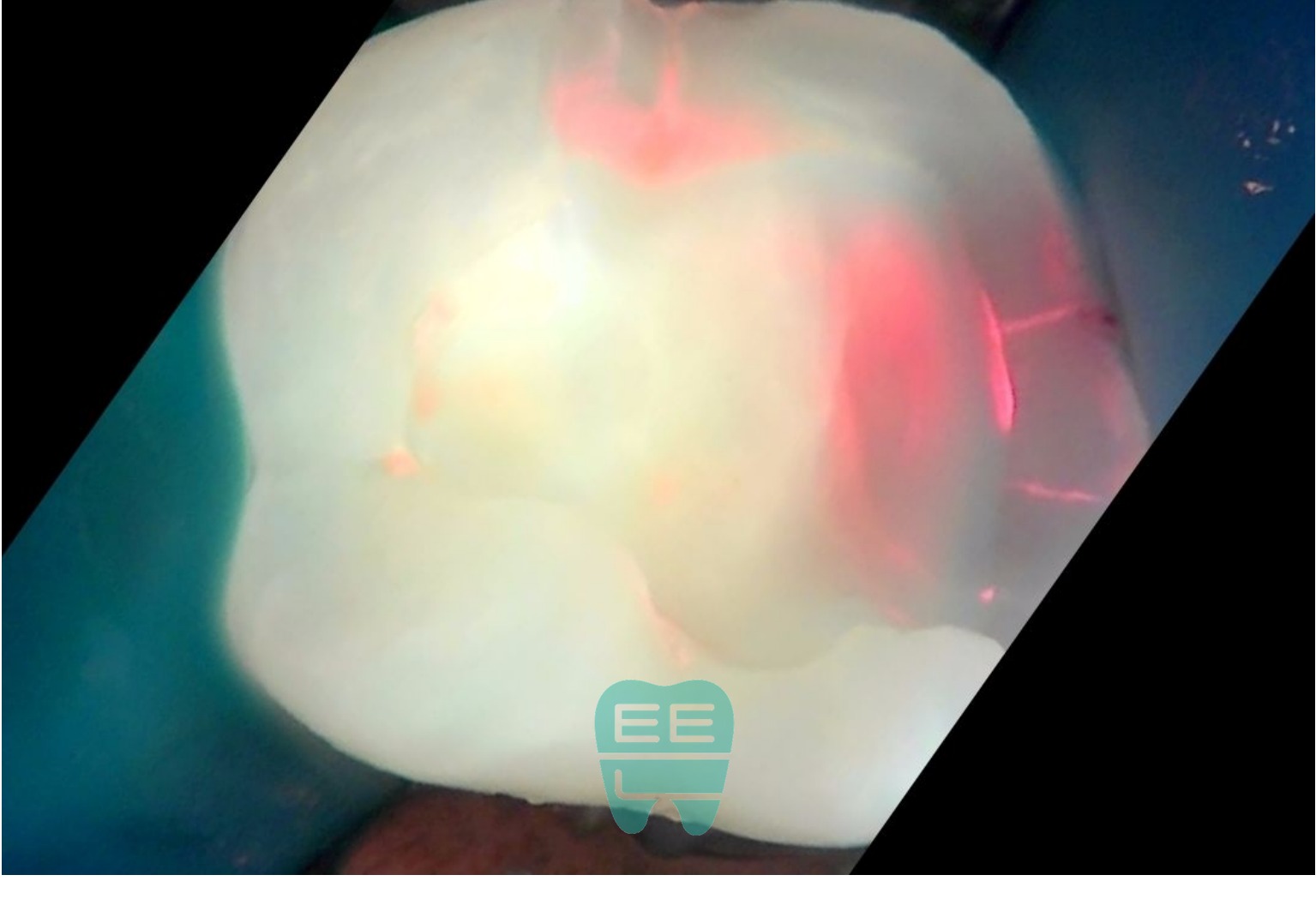
During the decay removal process, we re-check with Q-ray. Residual decay and contamination are still visible. Areas that are difficult to distinguish by eye can be objectively verified through Q-ray imaging.

After continued excavation, this Q-ray shows that residual decay and contamination have been significantly removed. By repeating Q-ray scans throughout the process, we objectively verify complete caries removal.
6. AquaCare Surface Treatment

After removing all decay, we treated the tooth surface with AquaCare. AquaCare's micro-powder spray removes any remaining microscopic contaminants and improves resin bond strength by up to 21% (per 2025 J Esthet Restor Dent study).
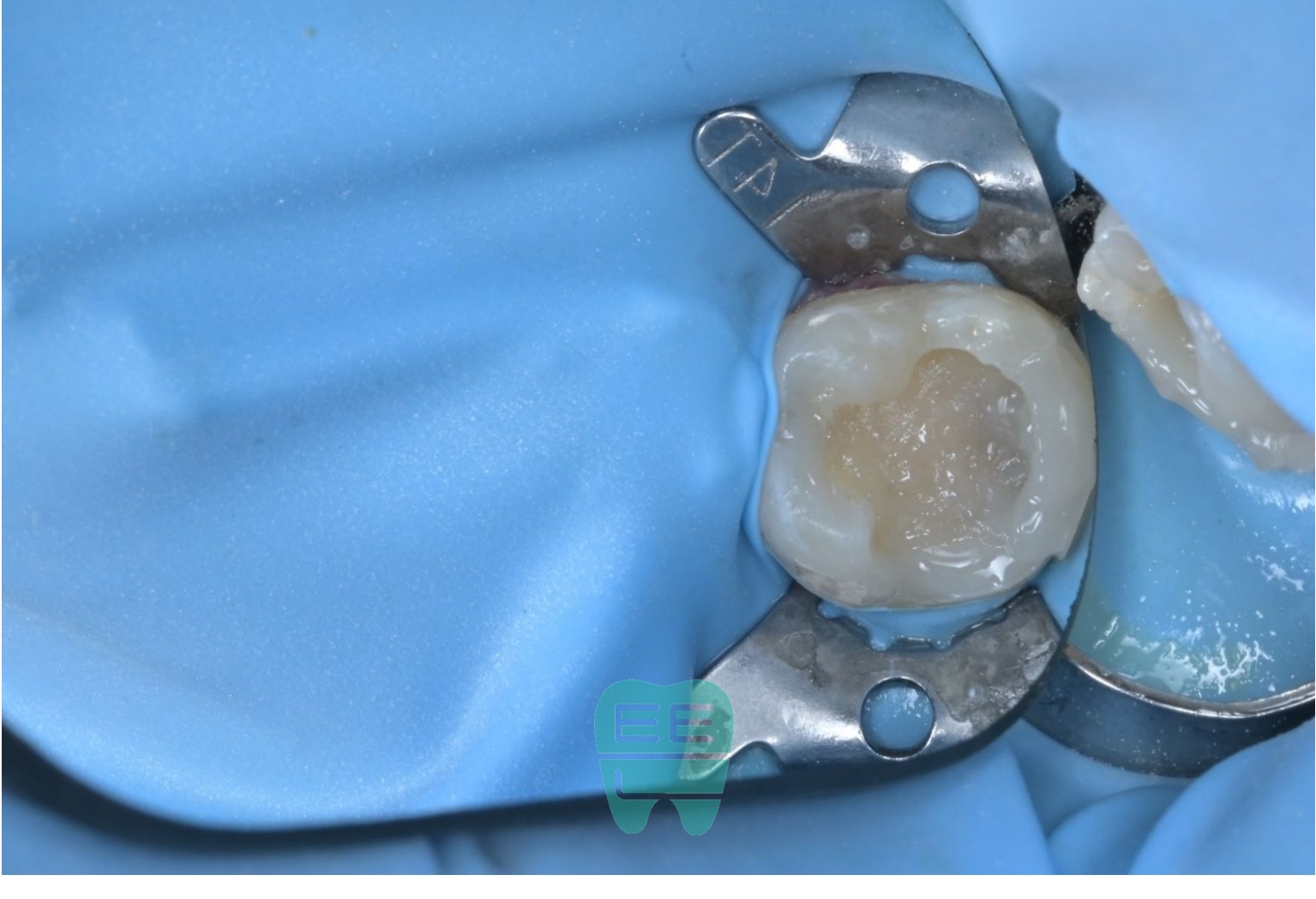
7. Ready for Bonding
Caries removal and surface treatment are complete. The tooth is ready for bonding — clean dentin is exposed and perfect moisture isolation is maintained by the rubber dam.
8. Fiber-Reinforced Resin Build-up
This is the critical step in today's treatment. Because the cavity was so extensive, simply filling with resin alone might not provide adequate strength. Fiber reinforcement dramatically improves the durability of resin in large restorations — it's an essential step.
While crowns and inlays require additional removal of healthy tooth structure, fiber-reinforced resin build-up preserves maximum healthy tooth while still achieving adequate strength.
9. Resin Build-up Complete
Using incremental layering technique under the dental microscope, we recreated the natural occlusal anatomy of the tooth.
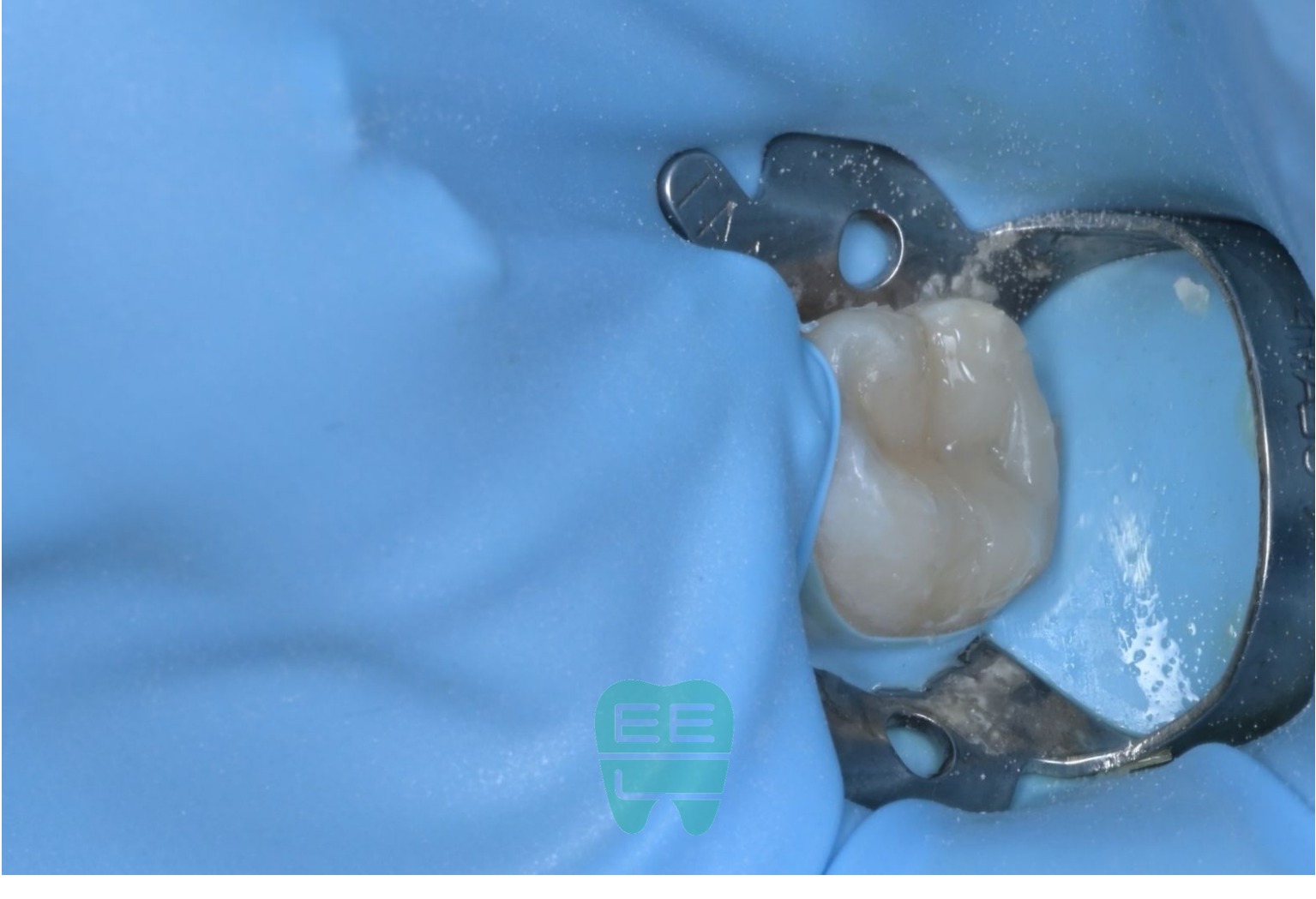
From another angle, you can see that proper three-dimensional contours have been restored.
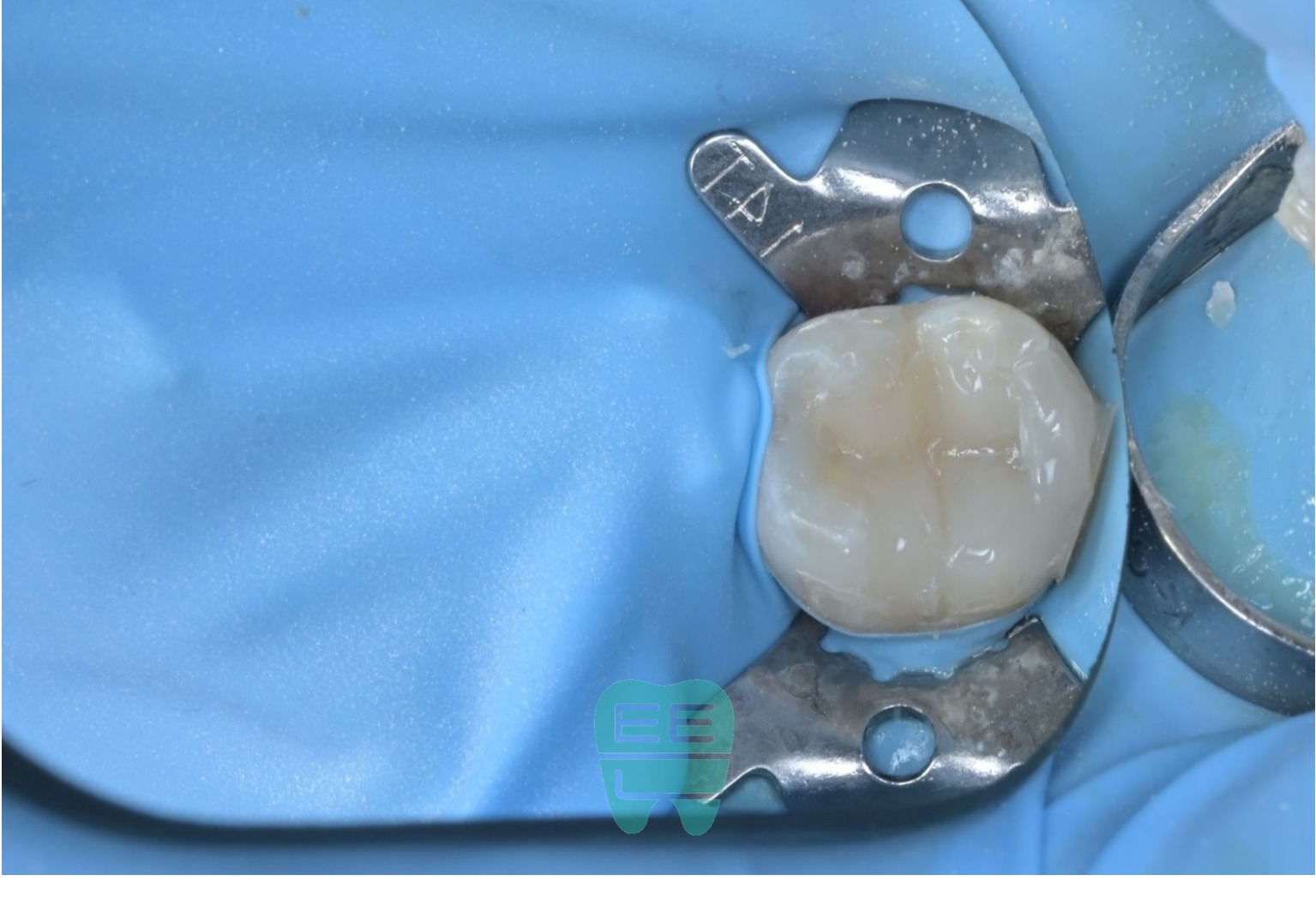
10. Treatment Complete: Occlusal Adjustment and Polishing



The final result after occlusal adjustment and polishing. Completely different from the debonded resin we started with. Natural shape and color that blends seamlessly with the surrounding teeth, with proper occlusion confirmed.
11. Post-Treatment Radiographic Verification

The post-treatment bitewing radiograph confirms proper contours. The interproximal anatomy is well-formed, and the resin is fully adapted with no voids underneath.
Why Minimally Invasive Resin Build-up for Children?
A 9-year-old's molar is a permanent tooth that needs to last a lifetime. Placing a crown at this age means:
- Additional healthy tooth structure must be removed for crown preparation
- It's difficult to adapt to occlusal changes as the child grows
- Every future crown replacement removes even more tooth structure
In contrast, minimally invasive resin build-up:
- Removes only infected tissue and preserves maximum healthy tooth
- Achieves adequate strength through fiber reinforcement
- Allows partial repairs, making future maintenance easier
- Minimal tooth reduction keeps future treatment options open
Just as no implant is better than your natural tooth, no crown is better than preserving more healthy tooth structure.
If you have questions about pediatric dental treatment, please don't hesitate to contact Shin Youngtong TTE Dental Clinic.
Shin Youngtong TTE Dental Clinic
- Address: 2F Golden Avenue, 66 Yeongtong-ro, Hwaseong-si, Gyeonggi-do, South Korea
- Phone: 031-205-4285
- Hours: Weekdays 10:00-19:00 / Wednesday late night until 21:00 / Saturday 10:00-14:00
임상 사진
(16장)Frequently Asked Questions
Children's permanent teeth are still growing, so aggressive treatments like crowns that require removing healthy tooth structure are disadvantageous long-term. Resin build-up removes only the infected area while preserving maximum healthy tooth, keeping future treatment options open.
Secondary caries occurs when the previous restoration had incomplete caries removal or poor bonding, allowing bacteria to infiltrate through micro-gaps. Using rubber dam isolation and dental microscopes during treatment significantly reduces this risk.
A rubber dam completely shields the treatment area from saliva and blood. Since resin bonding is extremely moisture-sensitive, treating without a rubber dam dramatically increases the risk of bonding failure and recurrent decay — especially critical for children who have difficulty controlling saliva.
AquaCare uses micro-powder air abrasion to remove residual contaminants and biofilm from the tooth surface. When applied after caries removal, it improves resin bond strength by up to 21%, significantly enhancing the longevity and seal of the restoration.
When a cavity is too large for resin alone to provide adequate strength, glass fiber is embedded within the resin to reinforce it. This technique achieves sufficient strength without additional tooth removal like crowns or inlays, making it particularly effective for pediatric molar restorations.
관련 증례

Same Cavity, Different Outcomes — How Dental Microscopes Transform Every Treatment

AquaCare: Scientific Evidence for Enhanced Bond Strength — 2025 International Research Review
